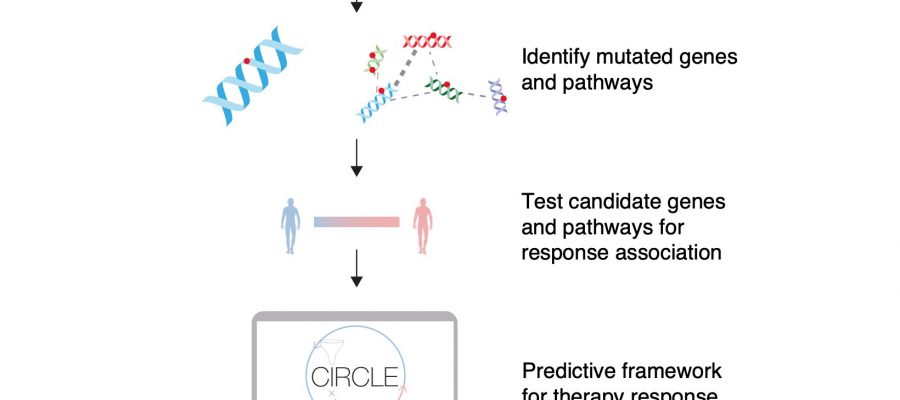
 Combine immunotherapy whole-exome sequencing datasets. 2) Identify mutated genes and pathways. 3) Test candidate genes and pathways for response association. 4) Predictive framework for therapy response (determining Responder or Non-responder). Credit: Sanjana and Imieliński Labs")
Immunotherapies, such as immune checkpoint inhibitors, have transformed the treatment of advanced stage cancers. Unlike chemotherapies that kill cancer cells, these drugs help the body’s immune system to find and destroy cancer cells themselves. Unfortunately, only a subset of patients responds long-term to immune checkpoint inhibitors—and these treatments can come at a high cost and with side effects.
Researchers have developed a two-step approach using whole exome sequencing to zero in on genes and pathways that predict whether cancer patients will respond to immunotherapy. The study, published in Nature Communications and conducted by researchers at New York University, Weill Cornell Medicine, and the New York Genome Center, illustrates how the use of whole exome sequencing can better predict treatment response than current laboratory tests.
“Can we better predict who will benefit from immunotherapy? Scientists have developed various biomarkers that help anticipate immunotherapy treatment response, but there’s still an unmet need for a robust, clinically practical predictive model,” said Neville Sanjana, assistant professor of biology at NYU, assistant professor of neuroscience and physiology at NYU Grossman School of Medicine, a core faculty member at New York Genome Center, and the study’s co-senior author.
Several biomarkers—including age, tumor type, and the number of mutations found in cancer cells, known as tumor mutational burden—are already known to correlate with responses to immunotherapy. Tumor mutational burden, which is calculated by analyzing a few hundred genes, is the most well-established predictor and is often used to determine a patient’s eligibility for immune checkpoint inhibitors.
If scientists look at a much larger portion of our genes, could that help to better predict which patients will respond to immunotherapy? Whole exome sequencing is a method for sequencing the part of the genome that codes for proteins—around 20,000 genes, or two percent of the genome—to look for mutations that may be involved in disease.
While whole exome sequencing is not widely used in cancer treatment, some recent studies of immunotherapies have started to include sequencing. These studies are small, but together can help illuminate the relationship between genomic factors and how patients respond to immunotherapy.
The researchers combined data from six previous immunotherapy studies of patients with melanoma, lung cancer, bladder cancer, and head and neck cancer. Whole exome sequencing was available for all participants, who were treated with an immune checkpoint inhibitor (either anti-PD-1 or anti-CTLA-4).
But even after combining the six studies, the number of patients—319 in total—was still relatively small.
“The problem with a small study of only a few hundred people is a mismatch between the number of patients and the vast number of genes sequenced in whole exome sequencing. We’d ideally have a dataset with more patients than genes,” said Zoran Gajic, a graduate student in the Sanjana Lab, and the study’s first author.
To get around this problem, the researchers turned to a model called fishHook which distinguishes mutations that drive cancer from background mutations, or mutations that occur by chance but are not involved in cancer. The model corrects for a range of factors that affect the rates of background mutations—for instance, adjusting for the size of a gene, since larger genes are more likely to have mutations.
Using this model, the researchers employed a two-step approach: first, they looked at the sequencing from all patients to find any genes with a higher mutational burden than they would expect, adjusting for genomic factors like gene size or whether a particular piece of DNA is a known hotspot that tends to accumulate more mutations. This yielded six genes with suspiciously high mutational burdens.
Next, the researchers determined if any of these six genes were enriched in people who responded or did not respond to immunotherapy. Two of the genes—KRAS, a gene often mutated in lung cancer, and BRAF, the most commonly mutated gene in melanoma—were enriched in patients who responded to immunotherapy. In contrast, two other genes—TP53 and BCLAF1—were enriched in those who did not respond to immunotherapy. BCLAF1 is not well studied, but these findings suggest that patients with BCLAF1 mutations are less likely to respond to immune checkpoint inhibitors.
Using the same two-step approach on collections of genes called pathways, the researchers determined that certain pathways (MAPK signaling, p53 associated, and immunomodulatory) also predicted immune checkpoint inhibitor response.
They then combined the four genes and three pathways with other predictive variables such as age, tumor type, and tumor mutational burden to create a tool they named the Cancer Immunotherapy Response CLassifiEr (CIRCLE). CIRCLE was able to better predict immunotherapy response by approximately 11% than tumor mutational burden alone. CIRCLE was also able to accurately predict cancer survival after immunotherapy.
“These results suggest that the use of broader diagnostics such as whole exome or even whole genome sequencing may significantly improve our ability to predict who will respond to immunotherapy—essentially, showing that more data does help to better predict treatment response,” said Marcin Imieliński, associate professor of computational genomics and associate professor of pathology and laboratory medicine at Weill Cornell Medicine, a core faculty member at the New York Genome Center, and the study’s co-senior author.
To validate their approach, the researchers tested CIRCLE on data from 165 additional cancer patients with whole exome sequencing who underwent treatment with immunotherapy and found that CIRCLE captured predictive information beyond that obtained from tumor mutational burden alone.
Future research will involve testing CIRCLE on larger cohorts of patient data, as the researchers anticipate that the model will improve with data from thousands of patients rather than hundreds. They also hope that with larger cohorts, they can begin to tease out which patients are likely to respond to different immunotherapies, given the growing number of treatments available.
Source: Read Full Article